

The Transgender Mirage


Introduction
Before the mid of the 20th century, no culture on the planet reassigned the sex of its individuals. The first experiments with attempts to reassign sex occurred in interwar Germany, and by the mid-20th century, clinicians working in North America created the concept of “transsexual.” By the late 20th century, a tiny proportion of the population of certain countries identified as transsexuals, and they changed their sex in their official documents. In recent decades the term transsexual fell in disuse and was replaced by transgender. Concurrently, there has been an explosion of the population in the Western Hemisphere that identifies as transgender.
Given the exponential increase in the numbers of people subjected to cross-sex hormones and surgeries, understanding how modern western society has arrived at this situation, historically without parallel in any previous culture, is becoming imperative. This article reviews the concept of biological sex and shows that transsexuality is essentially based on an incorrect concept of sex, which invalidates the concept of sex reassignment. This article shows that the concept of “gender identity” as distinct from biological sex is socially constructed.
This paper also argues that there exist two different subjective conditions associated with the concept of transgenderism: The first subjective condition is gender dysphoria, which is the desire to change sex. The second condition is the transgender identity, in which the individual develops a subjective belief regarding the category of their sex that is incongruent with biological reality.
This article proposes that the etiology of gender dysphoria is the concept of transgenderism in itself. If people view their gender as a datum, like their age, they will not desire to change it. The concept of sex reassignment, which conceptualizes that a person’s sex is malleable, provides the fertile ground required for gender dysphoria to develop. That is, what we consider the “gender affirmation” treatment for gender dysphoria is also the etiology for gender dysphoria. As changing biological sex is technically impossible, we conclude that “gender affirmation” treatment for gender dysphoria is a fraudulent medical product, and the existence of gender dysphoria is the consequence of the availability of this (fraudulent) product.
1. The reality of biological sex
Among mammals, there are two sexes: males who have XY chromosomes and produce small gametes and females who have XX chromosomes, produce large gametes, and whose body has the natural capacity to gestate offspring.
There exist a tiny minority of individuals (roughly 0.02%) who suffer from disorders of sexual development, such as Androgen Insensitivity Syndrome and Klinefelter Syndrome, and those individuals fail to fully meet the definitions of being a member of one of these two sex categories, so they are often called “intersex conditions” (see Soh (2020) for further details).
As of 2021, the current state of medical knowledge implies that it is impossible to change the biological sex of a human: for every individual, their biological sex is the same for their entire lives.
2. The concept of transsexuality is originally based on an understanding of sex on a spectrum
Harry Benjamin coined the term “transsexual” in his treatise of the subject “The Transsexual Phenomenon” (see Benjamin (1966)). When he coined the term, he implicitly denied what is now understood as the reality of biological sex. Instead, Benjamin claimed that sex had a set of components: genetic, anatomical, endocrine, psychological, and in each of these components, sex was a spectrum from total masculinity to total femininity. He was an endocrinologist who had been working for decades before the discovery of the DNA. Thus, his formulation of sex was quite distinct from our modern concept: According to his formation, a person’s sex was a state along a continuum of possible states of the same basic intersex human creature. It is similar to the understanding of the biological sex of the Ancient Greeks that males and females have the same fundamental anatomy, but females are “inverted” (see Joyce (2021)). For example, Benjamin defined the concept of “psychological sex” as a spectrum of how congruent an individual’s personality is with stereotypes of masculine and feminine personalities.
Thus, inside each human, he thought there was a template to make a male or a female. By varying their hormonal levels along a continuum from the female normal hormonal levels to the male normal hormonal levels, there is a continuum of different states of “endocrine sex.” Harry Benjamin also believed that anatomical sex was a spectrum, as he stated:
“Just as the anatomical sex is never entirely male or female (one must recall the existence of nipples in men and of a rudimentary penis, the clitoris, in women), so is the endocrine sex “mixed” to an even greater extent. Testes as well as the male adrenals produce small amounts of estrogen. Androgen, in more or less distinct traces, can be found in the ovaries and in larger amounts in the adrenals of females. Their metabolic end-products can be identified and measured in the blood as well as in the urine. Therefore it can well be said that, actually, we are all “intersexes,” anatomically as well as endocrinologically.
…
Consequently, the treatment with hormonal products (or surgical procedures) can make more or less distinct impressions on the endocrine sex, feminizing a male and masculinizing a female. This is an example of how one of the various “kinds of sex” can be deliberately altered.” (Benjamin 1966, page 8)
To Harry Benjamin, a “man” is not just an individual with XY chromosomes who produces small gametes, but an individual that fulfills a set of “masculine” social functions, appearance, dress, and behavior, and has a “masculine” psychological profile. In other words, in developing his concept of transsexualism, Benjamin was equating sex with sex-related stereotypes in appearance, presentation, and personality. We should note that in reality, nobody is perfectly congruent with this set of stereotypes that change across time and cultures. Thus, by Benjamin’s conception, everyone is transgender.
The idea that sex is not a binary biological datum but consists of a series of sex-related stereotypes and exists in a spectrum is widely endorsed by many individuals working in transgender medicine today. However, anybody familiar with the most fundamental aspects of modern biology understands that this is incorrect.
3. The concept of gender identity
It is a clear fact that the human sex is a biological datum: a reproductive function determined by the genetic material of each cell in the human body, given the absence of disorders of sexual development. It is also understood to be technically impossible to change the sex of a person given present technology. Therefore, every doctor understands that a true “sex-change” of an individual human being is impossible. Given this reality, how can we define gender identity as a distinct category from biological sex?
Human beings construct a subjective model of the world in their minds to form beliefs regarding the set of available choices and possible consequences of the choices that they can make. This subjective model of the world includes the individual’s perception of himself or herself. Regarding this subjective construct that we can define gender identity: Gender identity is the subjective perception of an individual regarding his or her sex.
A cisgender individual holds the subjective perception of their sex congruent with material reality: a male identifies himself as a male, a female identifies herself as a female. A transgender individual is an individual who holds the subjective belief that his or her sex is not his or her material sex. That is, we say that a transgender has a cross-gender identity. For example, Serano (2007) spoke about being male-bodied in her past and female-bodied when she wrote her book — writing as if her sex had changed. This subjective belief explains the concept of sex “assigned” at birth instead of sex “observed” at birth: the transgender individual disagrees with the sex diagnosis that doctors have observed. Thus, a transwoman is a human male who holds the belief to be a human female. A transman is a human female who holds the belief to be a human male.
A transgender person is a person who, by definition, has a subjective perception of their sex that is incongruent with material reality. Therefore, gender identity does not need to be related to this reality. Thus, the sex a transgender identifies as can be entirely fictional. This complete unmooring of subjective belief regarding material reality explains the proliferation of the nonbinary gender identities, which are fictional sexes besides male and female, such as “moongender” (identifies as the moon) or “treegender” (identifies as a tree).
As being transgender means a discrepancy between subjective beliefs and material reality, Stock (2021) has called being transgender a form of engaging in fiction. However, there is an important difference between engaging in fiction and the type of discrepancy between subjective beliefs and material reality that occurs in a cross-gender identity. When an individual is engaged in fiction, the individual is aware that the fiction is not real; they are aware they are engaging in suspense of disbelief. The transgender individual is different; in most cases, a transgender individual has serious difficulty in accepting that his or her gender identity is not real.
The word crossdresser describes individuals who perform the fiction of being the opposite sex with the full awareness that it is fictional. Some crossdressers even adopt fantasy names of the opposite sex when in character. Others go further and engage in permanent cosmetic treatments to alter their appearance toward the opposite sex, but they never believe their sex has changed.
One might include transgender individuals who disguise themselves as the opposite sex in daily life, trying to be perceived by others as the opposite sex. However, they have the correct perception of their biological sex. Instead of having a transgender identity, they effectively engage in deception by disguising themselves as the other sex to others. We define this type of cross-gender behavior as the Mulan-type pseudotransgender (in reference to the Chinese tale of the woman who disguised herself as male to serve in the army), as they lie to others about their sex but admit the truth to themselves. They are a midpoint between the crossdresser and the transgender. A crossdresser is not consciously attempting to be perceived by others as the opposite sex in daily life but engages in the performance of cross-sex-related stereotypes, typically as a part-time hobby. A transgender genuinely believes that their sex is the opposite of their biological sex.
4. The etiology of transgenderism: affirming the concept of gender identity creates gender dysphoria
Unlike physical illnesses such as cancer and Covid-19, mental illnesses are socially constructed; as Szasz (1961) famously argued, mental illness is a metaphor and not a medical illness in the technical sense. Instead of being discovered, the psychiatric profession creates mental disorders. Thus, cultural conditions determine what kinds of behaviors emerge and which we regard as mental disorders: As reported in Watts (2011), a set of specifically American types of mental illnesses has spread globally. Gender dysphoria is a mental disorder of North American origin, which also has spread globally.
Gender dysphoria is a desire to become a member of the opposite sex. It is regarded as a mental disorder when this desire becomes severe enough to impact daily life (in that sense, it is similar to a compulsive desire in the form of an addiction). As noted in Benjamin (1966) page 4: There exists a relatively small group of people — men more often than women — who want to “change their sex.” Note that the desire to change their sex is distinct from the belief of being of different sex to their biological sex, which is the condition of being transgender. Thus, the cross-gender identity occurs when a person develops the belief of being a member of the opposite sex to satisfy the desire to change sex.
This desire can, in principle, develop for various reasons (Blanchard and Bailey (2017) summarize a set of probable causes of gender dysphoria). This paper argues that, in principle, any person can develop the desire to become the opposite sex. To understand why this desire develops, consider the desire to consume chocolate. This desire has two conditions to manifest: the belief that there is such a food product called “chocolate” and the belief that choosing to consume this food product would increase welfare, that is, a shift from a less satisfactory state to a more satisfactory state.
The desire to change sex develops in an individual for essentially the same reason: It develops when the individual finds the idea of transitioning to the opposite sex to be beneficial. That is, gender dysphoria develops in an individual when two necessary and sufficient conditions on subjective beliefs are satisfied:
(1) The belief that changing sex is possible.
(2) The development of the belief that changing sex will improve the person’s welfare.
In other words, a person desires to change their sex if and only if (1) and (2) are satisfied. One important thing to note is that belief (1) is false, and belief (2) cannot be known since changing sex is fundamentally impossible: a man (woman) cannot form rational expectations regarding the benefits and costs of becoming a woman (men) since there exists no such thing. Thus, an important distinction between gender dysphoria and the desire to consume chocolate is that false beliefs are required for gender dysphoria to develop.
Gender dysphoric patients often describe a feeling of discomfort or distress regarding their sex. Patients often express their gender dysphoria as dissatisfaction with secondary sex characteristics, which are the physical manifestations of their sex. Suppose a person has developed beliefs (1) and (2) in their mind. In that case, that person will be under the constant state of perceiving their current life as being less satisfactory than the life they could have by “transitioning,” thus their mind will be under the constant perception that welfare could be improved by transitioning, which can lead to distress regarding their current sexed state and their secondary sex characteristics. It is analogous to the perception that a couch might be uncomfortable: This perception exists because the individual has beliefs regarding the existence of another couch that is more comfortable. In the same way, a person might feel their sexed body uncomfortable only if they believe that a custom-made body of the opposite sex, that they imagine to be more comfortable, can replace their current body.
Gender dysphoria is socially constructed: While factor (1) is biologically impossible, by decoupling gender from sex and stating that changing gender is possible, the medical profession created the perception that belief (1) is true. The belief (2) develops from the set of sex-related stereotypes of appearance and behavior that a person might think they can adopt by “transitioning” to another sex. Thus, gender dysphoria develops from a combination of the illusion of sex change as advertised by the medical profession with the perceived benefits of sex change, which are derived from socially constructed sex-related stereotypes in appearance, presentation, and behavior.
Historically there have been reports of people who wished to change their sex. For example, it was a common desire is for women to have been born male to be able to access male-only spaces in many historical societies where women had restricted rights compared to men. However, the idea that people can change their sex is very recent from a historical perspective: the first attempts at sex reassignment occurred in interwar Germany and it was only in the post-war US that there was a formal recognition of sex reassignment.
As information regarding the concept of changing sex being feasible is spreading around the population (that is, as internalized “transphobia” is being deconstructed), the number of transgender persons is increasing exponentially: Stock (2021) states that in the UK, the estimated transgender population increased from 3,000 to 5,000 in the early years of the 21st century to 600,000 by the end of the second decade of the 21st century. The explanation for this explosion is simple: More people have developed the belief that “changing their gender identity” is a choice variable, ignoring the biological fact that their sex is a datum. Thus, even if we assume as fixed the fraction of the population that might perceive changing their sex as beneficial, the spread in awareness of the concept of malleable sex generated an exponential increase in the number of people with a cross-gender identity.

Figure 1. The number of breast surgeries performed for sex reassignment in the US from 2015 to 2020. Source: American Society of Plastic Surgeons (ASPS).
An analogous situation to the mental illness of gender dysphoria would be the idea of mortality dysphoria: Consider the desire to become biologically immortal, that is, to live forever without aging. Biological immortality is a far more common human desire than to change sex. Consider the following situation: Suppose that doctors developed a treatment called “immortality transition,” where a mortal person could “transition” to an “immortal identity.” The treatment would be purely cosmetic: plastic surgery and perhaps hormone injections would be prescribed to create a youthful appearance and the illusion that the person is biologically immortal. However, doctors would also claim that the persons who undergo the treatment are immortal in an analogous fashion to the assertion that “transwomen are women.” Given how widespread is the fear of death, it would be expected that many people would feel “crippling dysphoria” from the reality of their mortality and would become obsessed with the idea of transitioning to an “immortal” identity. Like transwomen who believe they are women, “transimmortals” would live under the subjective belief of being immortals who were assigned as mortals at birth. Thus, “mortality dysphoria” would become a common mental illness treated with affirming an immortal identity through cosmetic treatments.
Thus, gender dysphoria has an etiology intrinsically originating from the medical concept of sex-change as a product of the medical industry, in the same manner as videogame addiction has an etiology originating in the existence of videogames supplied by the videogame industry. However, there is an essential difference between gender dysphoria and videogame addiction: Videogames exist in our present reality while changing a person’s biological sex does not.
4.1. Autogynephilia and the etiology of gender dysphoria
Historically, the majority of gender dysphorics were males (Benjamin (1966)). The dominant characteristic of male gender dysphorics is the presence of a paraphilia called autogynephilia. Autogynephilia is a common paraphilia in males, closely related to transvestism (Blanchard (1991) defines transvestism as a combination of fetishism with autogynephilia) is present in most gender dysphoric males.
Autogynephilia is an introverted manifestation of male heterosexuality, a fact that was already understood by Freund and Blanchard (1993) as “erotic target identity inversion”: Autogynephilia is a paraphilia where the male, sexually attracted to femininity, is erotically sensitive to internal in addition/ or rather than external stimuli. Thus, instead of finding their locus of sexual attraction in an external female person, the autogynephile is sexually aroused by the thought or image of himself feminized. This self-feminization consists of various types of cross-gender fantasies and behaviors, such as fetishes involving female clothing and appearance (transvestism), female anatomical features (anatomical autogynephilia), female physiological features (physiological autogynephilia), engaging in stereotypically feminine behavior, and being perceived as female by others.
The most common behavior for indulging in autogynephilic desires is transvestic fetishism: the use of clothes and makeup to make a male’s appearance feminized. It includes typically female clothes such as makeup, long hair, dresses, and heels, but it can also go much further and include the removal of body hair, a corset and petticoat to create an hourglass figure, and breast forms, combined they create the impression of the morphology of the female reproductive anatomy. For the more sophisticated crossdresser, a variety of prosthetic makeup products also exist, including prosthetic vaginas and full silicone bodysuits. Some crossdressers even have plastic surgery to look more feminine.
There are varied other methods for autogynephiles to indulge in their erotic desires and include indulging in gender-bending erotic fiction, the consumption of pornography featuring shemales (males anatomically feminized with plastic surgery, as the autogynephile, can self-insert as them), and impersonating a female character or a male character of feminine appearance in roleplaying games. Others consume conventional pornography made for heterosexual males but instead of consuming pornography by inserting themselves in the male perspective as it’s typical in straight males, they insert themselves in the female’s perspective during coitus (a clear manifestation of the erotic target identity inversion involved in this paraphilia).
Given the character of autogynephilic sexuality, it is not hard to understand that an autogynephile would be more interested in the concept of changing his sex if that option is presented to him than other male demographic groups: Blanchard and Bailey (2017) estimate that over 75% of cases of gender dysphoria in males are associated with the presence of autogynephilia at the time they wrote that article.
That does not mean that autogynephiles should develop gender dysphoria automatically. Instead, we might consider that a man with autogynephilia has a frame of mind that involves gender-bending fantasies. Therefore, such a man would have a frame of mind that is much more suggestive to considering the idea of changing sex than a typical heterosexual male. Thus, Blanchard (1991) remarked that virtually all heterosexual gender dysphorics had autogynephilia. Autogynephilia is not a sufficient condition for developing gender dysphoria, but it is one factor that might influence an otherwise typical heterosexual man to consider the concept of sex change.
Anne Lawrence (2007) stated that non-homosexual MtF transsexuals (typically autogynephiles) usually seek sex reassignment after some loss or reversal, such as the end of a meaningful relationship or unemployment and physical disability. For example, consider the case of depression caused by some such event in a male. If he is a typical heterosexual male, a sex change would never cross his mind during such a depressive episode, but if he is an autogynephilic male, then at that point, a sex change might be perceived by his mind as an effective form of overcoming his depression.
Nevertheless, the choice of undergoing the process of sex reassignment in the case of autogynephiles has a significant issue: Their desire for changing sex has roots in an erotic desire, but the process of sex reassignment destroys their sexual organs, and thus most of their sexual function. That is, in an ironic twist of fate, the case of a heterosexual man who is erotically attracted to the idea of achieving a more feminine appearance, ends up castrating himself due to his paraphilia, as stated in the following account by Danielle Berry:
I can speak the transgender party line that I was a female trapped in a male body and I remember feeling this way since I was 4. But, it’s never that easy if you look at it sincerely and without preconception. There’s little question that a mid-life crisis, a divorce and a cancer scare were involved in at least the timing of my sex-change decision. To be completely honest at this point (3 yrs. post-op) is not easy, however, I’m not sure I would do it again. I’m now concerned that much of what I took as a gender dysfunction might have been nothing more than a neurotic sexual obsession. I was a crossdresser for all of my sexual life and had always fantasized going fem as an ultimate turn-on. Ironically, when I began hormone treatment my libido went away. However, I mistook that relief from sexual obsession for validation of my gender change. Then in the final bit of irony, after surgery my new genitals were non-orgasmic (like 80% of my TG sisters). (Berry (2008))
A critical feature of autogynephilia is that the autogynephilic man does not need to believe to be a woman to satisfy his autogynephilia. Male sexuality is driven mainly by visual and tactile stimuli. In the case of autogynephilia is the stimuli of femininity in the self. Therefore, the satisfaction of autogynephilic desires does not require that the autogynephile develops a cross-gender identity. Instead, it requires the satisfaction of the specific fetishes as autogynephilia tends to manifest in various ways in different individuals:
· Some individuals have a mainly transvestic variant of autogynephilia, which can be satisfied by clothing and external prosthetics alone.
· Other individuals might find plastic surgery the most effective means to satisfy their autogynephilia (particularly true in cases of anatomical autogynephilia that might not be satisfied with non-invasive methods).
· Other individuals might require others to pretend they are female to validate their sexual fantasy (interpersonal autogynephilia).
In all cases, it does not require them to conceptualize themselves as female, just like enjoying a movie does not require the viewer to believe the movie to be real. Therefore, the development of a cross-gender identity is not required to satisfy any form of autogynephilia.
5. On the concept of gender identity being inborn and its relationship with gender dysphoria
A widespread belief in western culture today is that people have an inborn and immutable gender identity. This belief has the following implication: In almost everyone, their inborn gender identity is congruent with their biological sex, which means they have a correct subjective evaluation of their sex. In some cases, however, persons are born with an incorrect subjective perception of their sex. In this conception, a transgender person has a hardwired subjective perception of themselves in the brain that prevents them from identifying their sex correctly. The expression “being born in the wrong body” encapsulates this belief.
However, this notion that transgender people have an inborn cross-gender identity in the brain has already been falsified in clinical settings by Harry Benjamin in 1966. The patients with gender dysphoria Benjamin examined did not have a cross-gender identity. Instead, as Benjamin describes, these patients were aware of their biological sex, and instead of having a cross-sex identity, they just wanted to change their sex to the opposite sex. That is, gender dysphoria is the desire to change sex and is not an incorrect subjective perception of their sex. After sex reassignment surgeries, the patients develop the belief that they changed their sex: The transgender identity is created by the doctors, not by the patients. In addition, the concept of a person having an inborn gender identity does not explain gender dysphoria: if a man is born believing himself to be a woman, why would he develop the desire to become a woman if he is already one in the first place?
One could argue that while cross-gender identity is not inborn, gender-dysphoria is an inborn condition, but as shown in Singh et al. (2021), the vast majority of cases of childhood-onset gender dysphoria resolve during puberty. Therefore, neither cross-gender identity nor gender-dysphoria is inborn.
In addition, the concept of “inborn gender identity” reinforces sexist stereotypes: That persons have “female” or “male” minds as if there is such a thing Benjamin termed “psychological sex,” and transgenders are persons whose sexed minds do not “fit” their sexed bodies. Males and females indeed have different distributions of personality traits. Nevertheless, no single individual fits perfectly with the typical personality profile of the average male or average female. The degree of the incongruence of an individual with the median personality of their sex is not a good predictor of the development of gender dysphoria. Consider the case of male gender dysphorics. Autogynephiles are the majority of male gender dysphorics, and they tend to be stereotypically masculine men before they choose to transition to a cross-gender identity. It is also evident that most feminine men and masculine women do not develop gender dysphoria.
6. The reality of medical sex reassignment
The “sex reassignment” or “gender affirmation” treatment for gender dysphoria consists in the development of the belief that the patient has changed their sex. This belief is produced by a ritual called gender transition, which consists of a series of cosmetic and social procedures. The ritual of gender transition consists of series of surgical and hormonal interventions with purely cosmetic purposes with the objective to make it appear as if they are of the opposite sex and the patient is socially inserted as if they are of the opposite sex. In other words, to treat the condition of the individual that wants to change their sex, the treatment consists in the affirmation of the belief that they can change sex and a series of procedures organized as a ritual to produce the belief of a sex change.
The reality of medical transition is far from the idealization of sex change not only in biological terms as it is true as well as in cosmetic terms. There does not exist a standardized medical gender transition treatment, and different doctors prescribe different surgeries and cross-sex hormones recipes. These procedures are all done for purely cosmetic reasons although there is a substantial price to be paid in terms of physical health for their execution. The most typical procedures consist of chemical castration (“cross-sex hormone replacement therapy”) and the amputation of reproductive organs (“gender confirmation surgery”). Other common procedures include the modification of the patient’s skeletal structure (“shoulder reduction surgery”), and the patient’s skull shape (“facial feminization surgery”).
Analogous to what we can expect from a cosmetic treatment with the objective of making a 70-year-old person look like a 20-year-old, these cosmetic treatments designed to make patients appear to change their sex typically have poor results relative to their objective. The reality is that males and females have different anatomy in terms of body proportions and the basic body structure of patients is not changed by either superficial cosmetic treatments focused on small parts of the body or by hormonal treatments. So, unless these persons have natural body proportions that are exceptionally close to the opposite sex, it is typically self-evident that transgender people are not of the sex they claim to be.
The degree to which transgender individuals can disguise their sex varies between male to female individuals and female to male individuals. Unlike male to female individuals, female to male individuals often successfully disguise their biological sex to others. This asymmetry is due to two reasons: the ingestion of cross-sex hormones has much more potent effects in terms of masculinizing a woman than in terms of feminizing a man, as well as the curious fact that by using clothing and makeup, women can be more easily disguised as men than men can disguise themselves as women. For example, Norah Vincent lived disguised as a man for a year (technically being a Mulan-type pseudotransgender during this period), using only clothing and makeup, and she reports that others have never discovered her sex (Vincent (2007)).
The amputation of healthy body parts and the continuous injection of cross-sex hormones into an otherwise healthy body results in a severe deterioration of the patients’ health. Following transgender patients for 30 years, the study of Dheje et al. (2011) is, to the best of my knowledge, the only rigorous survey of the health outcomes of sex reassigned individuals over the long run. This study shows that the crude mortality rate of sex reassigned patients in Sweden was 2.8 times higher than in the general population, matched by demographic characteristics. This high death rate was driven partly by high suicide rates, which were 19 times the general population, the remainder being deaths from cardiovascular illness and cancer, both of which were much higher among gender affirmed patients than in the general population.
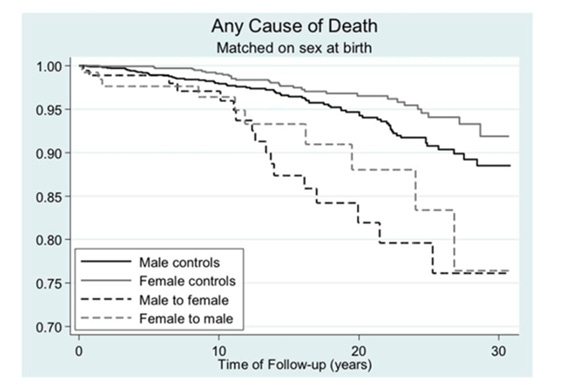
Figure 2. From Dheje et al. (2011), death from any cause as a function of time after sex reassignment among 324 transsexual persons in Sweden (male-to-female: N = 191, female-to-male: N = 133), and population controls matched on birth year.
What is the name for the situation when a company sells a product advertised as X, and it is Y? The name is fraud. Thus, “transgender medicine,” by continuing to exist after the medical profession understands that it is impossible to change sex with hormones and surgeries, is a fraud. The current phenomenon of selling cosmetic surgeries and hormones as “sex-change” is akin to marketing a horse-drawn wagon as a “high-technology Co2 emissions-free car with an organic engine”.
Thus, “gender affirmation treatment” consists purely of cosmetic treatments with severe costs in terms of physical health. American medical associations indeed support gender affirmation as the best treatment for gender dysphoria. That is expected: car sales association would also support car purchasing affirmation as the best treatment for the desire to purchase cars. Like cars, sex change is a product, and gender dysphoria is the desire to consume this product. However, there is a fundamental difference between gender affirmation and cars: gender affirmation is a fraudulent product.
The understanding that sex cannot be changed leads to the development of what we can call gender identity ideology (a term used by Joyce (2021)): since “transition” is understood to be just a ritual transgender people should be accepted as the gender they subjectively perceive themselves to be. What matters for determining whether a person is a male or female is only their subjective belief, with no medical transition required for affirming their gender. Under this ideological system, “women” means “persons who call their gender women.” The concept of gender loses absolutely all descriptive power and becomes an entirely vacuous identity: Under this ideology, knowing a person’s gender yields as much information about that person as knowing their astrological sign.
7. The transgender spiritual and ideological belief system
Given that changing sex is biologically impossible, the transgender population has developed a sophisticated set of spiritual beliefs regarding the meanings of “masculinity” and “femininity” to provide foundations for their cross-gender identity. For example, Serano (2007) provides an excellent example of the degree of sophistication a transgender person can develop their set of spiritual beliefs regarding sex-related stereotypes to provide the foundation for their cross-gender identity.
We can describe the transgender spiritual belief system as follows: It states that every person has a sexed soul, and when the sex of the person’s soul does not match the sex of their body, they are said to be “trans” or “born in the wrong body.” Those who subscribe to this belief system believe that when a person is born “trans”, they will develop gender dysphoria as a permanent condition whose only treatment is gender transition. Thus, gender transition is conceived as a process where gender dysphoric individuals find their “true selves.”
The concept of gender identity has spread through internet communities. As the internet allows for instantaneous communication while allowing individuals to become less associated with the material reality of their bodies by interacting through avatars, it has dramatically accelerated the social spread of gender dysphoria. According to this system of beliefs, congruence with a somewhat arbitrary set of sex-related stereotypes determines a person’s actual gender and not biology: Since no one can be perfectly congruent to a set of sex-related stereotypes, any person might conclude that they are “trans,” thus a person “born in the wrong body.”
The diffusion of these spiritual concepts has created the potential for a large group of people to start to believe that they might be “trans.” The reasons can be wide-ranging. For example, a heterosexual crossdresser who is sexually aroused when performing his female cosplay might start to believe he has a female soul. A stereotypically feminine man or a stereotypically masculine woman might also believe they have been assigned the wrong body at birth for just not conforming to their sex-related stereotypes. The members of the trans cult tend to regard any form of erotic crossdressing and gender non-conforming behavior as a sure sign that such individuals are “trans,” and they regard just the evidence of interest in the transgender belief system as a piece of solid evidence that person was “born in the wrong body.” Thus, if these individuals do not undergo the process of “gender transition,” they are labeled by the members of the trans belief system as “repressors.”
A set of activists and organizations can be regarded as the “transgender rights movement” who are aggressively advocating for imposing this spiritual belief system on society. This set of beliefs, if approached in this way, can be labeled as an ideology because it ceases to be only a spiritual belief system, like a religious cult that one can choose to participate in, but instead, a set of principles that describe how society should be organized.
In that regard, the trans movement is fundamentally distinct from major religious organizations: Other religious organizations tolerate persons of other religious beliefs and do not need to impose their beliefs in the form of law. Instead, the trans rights movement can be understood as being engaged in a spiritual struggle to impose their beliefs on the rest of society. This is incompatible with religious liberty: a man has the right to believe he is a “woman on the inside,” but he does not have the right to impose his belief on others.
8. Transgenderism, homosexuality, and the gender-nonconforming demographics
The conditions of transgenderism and homosexuality are not related on a fundamental level: Homosexuality is the sexual attraction to the same sex, while transgenderism is the manifestation of cross-gender identity. Transgenderism is, however, statistically related to unconventional sexuality due to the positive correlation of transgender identity and autogynephilia in males and transgender identity in females with homosexuality.
This paper hypothesizes that these correlations result from a culture that does not allow individuals to express themselves in incongruent ways to sex-related stereotypes, so these individuals must induce a cross-gender identity in themselves to express themselves naturally.
The critical point to be made is regarding the strictness of socialized gender roles in society. If a man likes wearing dresses and makeup and society is perceived as tolerant of this kind of behavior among men, then gender dysphoria would not arise in cases of gender non-conforming behavior and presentation. In fact, under a genuinely liberal culture, a man (woman) should be able to choose to have cosmetic surgeries to achieve a more feminine (masculine) appearance without having to question his (her) identity as a man (woman). Gender identity would be fundamentally determined by biological reality and not by sexist stereotypes regarding appearance and behavior.
A society that assigns a label of transgender to behaviors that do not conform to stereotypes of each sex is far from being a progressive society. Instead, such a society is fundamentally regressive because attaching the “trans” label to gender non-conforming behavior dehumanizes people who transgress sex-related stereotypes instead of allowing individuals to express themselves as individuals regardless of the degree to which they conform to sex-related stereotypes.
In some cultures, male demographic groups exist, such as the hijras in the Indian Subcontinent or the travestis in Brazil, which are considered individual members of their biological sex that do not conform to their culture’s sex-related stereotypes regarding behavior and presentation. In their culture, they are not understood as individuals who “transitioned” to be members of the opposite sex to the sex they were born. Despite attempts at conflation, these groups are a distinct demographic from the western concept of transgender people, which means a group of people who has a subjective perception of their sex incongruent with the material reality of their biological sex.
9. The prevention of gender dysphoria
If video games did not exist, psychologists would not need to treat patients with video game addiction. Analogously, gender dysphoria is the subjective perception of discomfort with the individual’s biological sex induced by the idea that changing their biological sex would improve comfort. The diffusion of a fraudulent idea causes this type of mental condition: The idea that changing sex is possible, when in fact, it is not.
Therefore, the prevention of gender dysphoria in the population can be achieved by suppressing beliefs (1) and (2). Belief (1) can be corrected by educating the population that sex change is biologically impossible. Belief (2) can be corrected by proper understanding that members of each sex can present and act without constraining themselves to sex-related stereotypes.
Autogynephilia should be understood as a sexual orientation like homosexuality and heterosexuality. Perhaps adopting a more inclusive term such as autosexual to describe autogynephilia and other forms of autoerotic paraphilias and its widespread use would improve social acceptance and understanding of human sexual variation. For example, a man with autogynephilic sexuality who alters his appearance through cosmetic surgery to feminize himself should be regarded not as a transwoman but as an autosexual man who is expressing his sexuality. Like a man with a homosexual orientation should be understood to be a gay man expressing his masculine sexuality, he is not a woman’s soul in a male body (as gays are often understood to be among the uneducated).
A truly progressive society is a society that allows members of each sex to be themselves without having to pretend they are not members of their biological sex. Instead, by emphasizing that any cross-sex stereotypical behavior is a sign of transgenderism, society has dramatically increased the number of people with gender dysphoria. Thus, the “gender affirmation” pandemic has been created by society’s failure to accept persons who do not fit with their sex-related stereotypes.
10. Conclusion: prudish culture and the transgender mirage
Mid-20th century America was a society characterized by prudishness and religiousness; it is no coincidence that transgender ideology, the disconnection of gender identity from biological reality, has first developed during that time and place. For individuals to escape the shackles of strictly defined gender roles in such a conservative society, the only way out appeared to be developing the belief of being a sexed soul trapped in a body with incongruent sex.
Today, the transgender rights movement appears to be primarily composed of autosexual men (see Joyce (2021)). Instead of facing the reality that they are men with a distinct sexual orientation, they adopt and advocate for the spiritual idea that they have somehow a female soul trapped in a male body. Thus, sexual shame appears to be a considerable component that fuels this ideology. Autosexual men tend to accept their erotic nature in other, less prudish cultures, often engaging in crossdressing as a part-time hobby. They live out their lives without feeling a compulsive need to live immersed in the belief of being a member of the opposite sex. That was the case before American cultural influence began to assert itself more strongly. Thus, the transgender mirage began in America but became a global pandemic.
This article argued that the transgender phenomenon is derived from the concept of sex change. While doctors have admitted that changing biological sex is impossible, broader society has not fully digested the implications of this information. Instead, the falsehood that changing sex is possible is promoted in the form of “gender affirmation.” Even Harry Benjamin has recognized the fact that transgender medicine is fundamentally a fraudulent enterprise: “As we have seen, these persons, in a strictly scientific sense, fool themselves. No actual change of sex is ever possible.” Benjamin, 1966, page 30.
Given the exponential increase in the number of people referred for “gender affirmation” surgeries, the health issues of “gender transition” treatments are becoming a public health problem. The populations with transvestism (estimated to be 3% to 8% of the male population, 1% to 3% in the female population, see Långström and Zucker (2005) and Joyal and Carpentier (2017) for lower and upper bound estimates, respectively) and homosexuality (roughly 4–5% of the male population, less than 3% of the female population, see Diamond (1993)) are particularly prone to developing gender dysphoria since transvestism is a manifestation of autosexual orientation and homosexuals tend to be gender non-conforming. Thus, globally, the population particularly vulnerable to developing gender dysphoria is in the hundreds of millions.
Like other religious beliefs, transgender identities should be respected, but the medical reality that gender dysphoria is a social construct and that the cosmetic treatments involved in gender affirmation are hazardous should not be denied. We should consider that, given the enormous health risks involved with gender affirmation, that the excess in mortality by subjecting a large population to gender affirmation treatments over the next few decades would be comparable to the excess mortality caused by a significant pandemic, such as the Covid-19 pandemic in 2020–2021. Thus, reducing the risk factors for the development of gender dysphoria should be considered in formulating public health policies.
It appears that our current concept of transgenderism exists in a midpoint in the process of relaxation of sex-related social norms: to label sex-nonconforming individuals as transgender is a concept that exists between a society where presentation and behavior are strictly determined by sex (like mid-20th century America) and a society where individuals do not need to conform to sex-related stereotypes.
References
Benjamin, Harry. The Transsexual Phenomenon. 1966. Julian Press, United States.
Berry, Danielle. Special Note to Those Thinking About a Sex Change. 2008. https://vickiedavis.blogspot.com/2008/10/special-note-to-those-thinking-about.html (accessed in 08.04.2021)
Blanchard, Ray. Clinical observations and systematic studies of autogynephilia. 1991. Journal of Sex and Marital Therapy. Volume 17, Issue 4, pp. 235-251.
Blanchard, Ray, and Michael J. Bailey. Gender Dysphoria is Not One Thing. 2017. https://4thwavenow.com/2017/12/07/gender-dysphoria-is-not-one-thing/ (accessed in 07.31.2021)
Diamond, Milton. Homosexuality and bisexuality in different populations. Archives of Sexual Behavior. 1993. Volume 22, pages 291-310.
Dhejne, Cecilia, Paul Lichtenstein, Marcus Boman, Anna L. V. Johansson, Niklas Långström, and Mikael Landén. Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden. PLoS One. 2011 Feb 22;6(2):e16885. doi: 10.1371/journal.pone.0016885. PMID: 21364939; PMCID: PMC3043071.
Freund, Kurt and Ray Blanchard. Erotic Target Location Errors in Male Gender Dysphorics, Paedophiles, and Fetishists. The British Journal of Psychiatry. 1993. Volume 162, Issue 4, Pages 558 – 563.
Henrich, Joseph. The WEIRDest People in the World: How the West Became Psychologically Peculiar and Particularly Prosperous. 2020. Farrar, Straus and Giroux, United States.
Långström, Niklas and Kenneth J Zucker. Transvestic Fetishism in the General Population: Prevalence and Correlates. Journal of Sex and Marital Therapy. 2005. Volume 31, Issue 2, Pages 87-95.
Lawrence, Anne. Becoming what we love. Perspectives in Biology and Medicine. 2007. Volume 50, number 4, pages 506-20.
Joyal, Christian C. and Carpentier Julie. The Prevalence of Paraphilic Interests and Behaviors in the General Population: A Provincial Survey. Journal of Sex Research. 2017. Volume 54, Issue 2, Pages 161-171.
Joyce, Helen. Trans: When Ideology Meets Reality. 2021. Oneworld Publications, United Kingdom.
Serano, Julia. Whipping Girl. 2007. Seal Press, United States.
Singh, Devita, Susan J Bradley, and Kenneth J Zucker. A Follow-Up Study of Boys With Gender Identity Disorder. 2021. Frontiers in Psychiatry. Volume 12, March Issue, Article 632784.
Soh, Debra. The End of Gender: Debunking the Myths about Sex and Identity in Our Society. 2020. Threshold Editions, United States.
Stock, Kathleen. Material Girls: Why Reality Matters for Feminism. 2021. Fleet, United Kingdom.
Vincent, Norah. Self-Made Man: One Woman's Year Disguised as a Man. 2007. Penguin Books, United States.
Watters, Ethan. Crazy Like Us: The Globalization of the American Psyche. 2011. Free Press, United States.
This is a well-written and well-argued article that offers some interesting analytical insights into the transgender phenomenon. Of particular interest is the viral nature of American ideas, which the Internet has empowered to spread around the world, particularly to Europe. It is a sort of Montezuma's Revenge, if you'll pardon the pun, that American neo-progressive ideas are colonising Europe so readily, not just with gender ideology but also with notions of white supremacy and a very American-style racialism.
Of course, as more and more people undertake the treatments on offer (especially children, and especially those children who show a sudden emergence of the phenomenon), there will be a larger and larger share of people who regret undertaking permanent life-altering medical interventions. It remains to be seen if the edifice crumbles under the weight of its own contradictions...or, rather, it remains to be seen how long this process takes, since it is as inevitable as the downfall of any religion.